Case study of a patient with Triple Vessel Disease undergoing PCI to LAD

CLINICAL PRESENTATION
Mr. O. S. a 71-year-old male, was admitted to the hospital with symptoms such as breathlessness, restlessness, intermittent dyspnea and angina on exertion along with generalized weakness. He is a known case of hypertension, Type 2 Diabetes Mellitus, Benign Prostatic Hyperplasia (BPH). Patient was advised for coronary angiography based on ECG and 2D echo report.
CORONARY ANGIOGRAPHY REPORT
RISK FACTORS
• Hypertension
• Type 2 Diabetes Mellitus
ECG
• Normal sinus rhythm
• Early repolarization in inferior leads
2D ECHO
2D echo: Normal cardiac valves & chambers.
Trivial MR. No regional wall motion
abnormality. Normal LV systolic function,
LVEF – 60%. Grade – I LV diastolic dysfunction,
Trivial TR.
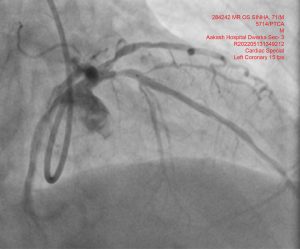
Left Anterior Descending Artery – Proximal
Tubular Calcific 80% Diseased; Early Di-Ostium
clean.
Post Ostial 60-70% Diffuse Disease
Highlight Bold – Co-Dominant, Diffuse Plaquing
Bold – Tubular 80-90% Disease
Right Coronary Artery – Co-Dominant, Proximal
to Mid Tubular Disease Maximum 90%
FINAL DIAGNOSIS
• Triple vessel disease
RECOMMENDATION
• CABG v/s multi-vessel PCI
Procedure done – Patient opted for PCI. He was taken up for Percutaneous Coronary Intervention (PCI)
and Left Anterior Descending Artery (LAD).
Initially Wolverine Cutting Balloon was used but after multiple dilatations it did not help much. Then
high-pressure balloon OPN NC 3 x 10 was used, and lesion was successfully dilated at 30 ATM.
PRE-PROCEDURAL FINDINGS






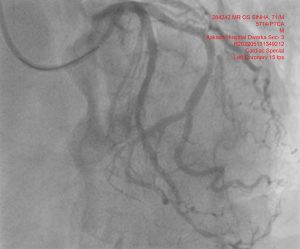
DETAILS OF INVESTIGATION (FINDINGS) POST PROCEDURE:
POST PROCEDURE MANAGEMENT
Post procedure period was uneventful. Patient was later managed with anti-platelets, statin, anticoagulants,
betablockers, antianxiety, antacids, and other supportive measures.
CONDITION AT THE TIME OF DISCHARGE
Patient improved symptomatically and was discharged in a stable condition with all vital signs and
other parameters within acceptable range and with plan for staged PCI. Pateints is doing well on Medical
Therapy
FOLLOW-UP
• Follow-up after 7 days in Cardio OPD with prior appointment with Dr. Amit Pendharkar/Dr. Aayush
Singal with CBC and KFT reports.
• Report in emergency department in case of chest pain or difficulty in breathing, syncope or severe
headache or any active bleed from any site.
DISCUSSION
• Three-vessel disease (3VD) is the most severe form of coronary atherosclerosis and patients with
3VD and/or left main stenosis are considered a high-risk group. As compared to less severe forms
of CAD, 3VD is consistently associated with worse long-term prognosis.1
• Many a times, the coronary lesions turn calcific and can become a rigid obstacle to optimal balloon and stent expansion. The conventional non-compliant (NC) balloons reach is 20 to 30 ATM
limit that can be insufficient. Thus, when conventional NC balloons fail, the new high-pressure
OPN NC balloon provides an effective and safe alternative strategy for the dilatation of rigid
coronary lesions.