Case study of a patient with triple vessel coronary artery disease undergoing PTCA with graft stenting

Clinical Presentation
Coronary Angiography Report
Risk Factors
- Hypertension
- Type 2 diabetes mellitus
ECG
- Sinus Rhythm
- T wave inversion V1 – V4
- Good LV systolic function
- AO/LVEDP/PCWP: 160/80/107
Approach – Right femoral
Catheters
- 5F JL
- JR 3.5
Contrast Media
- Contrast – Omnipaque
- Quantity – 50 ml
Flurotime: 7.29 Min
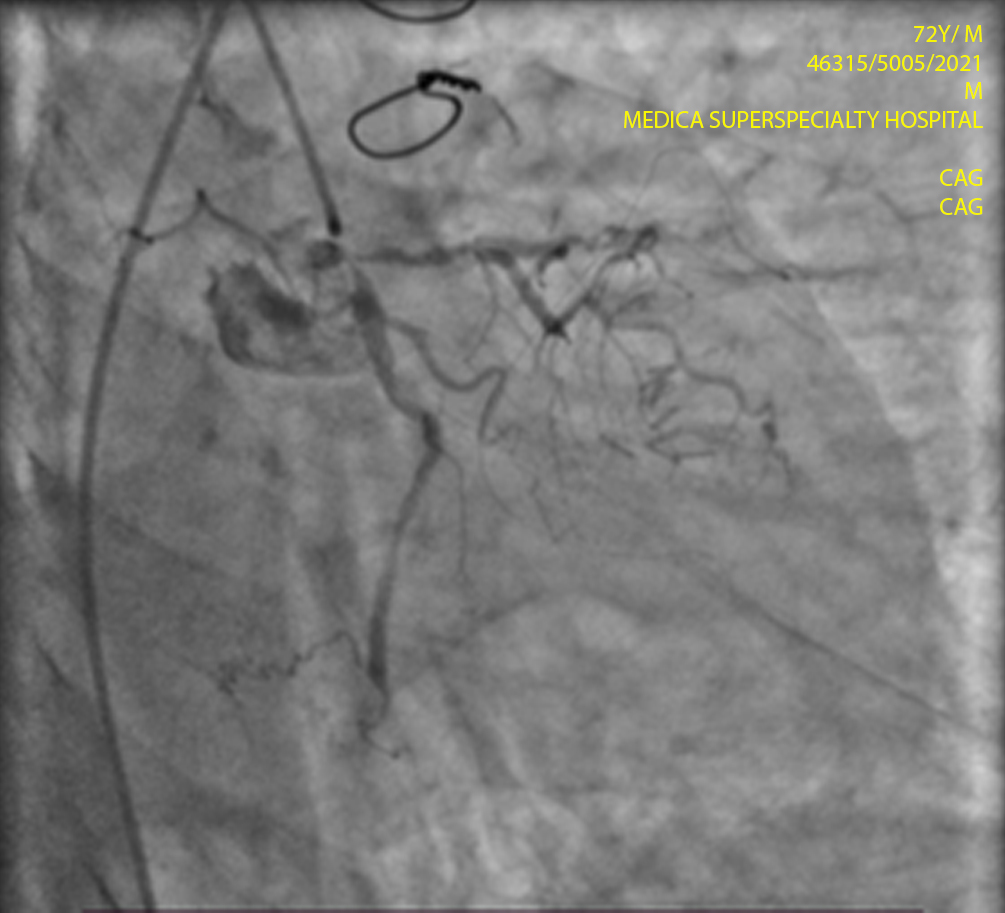
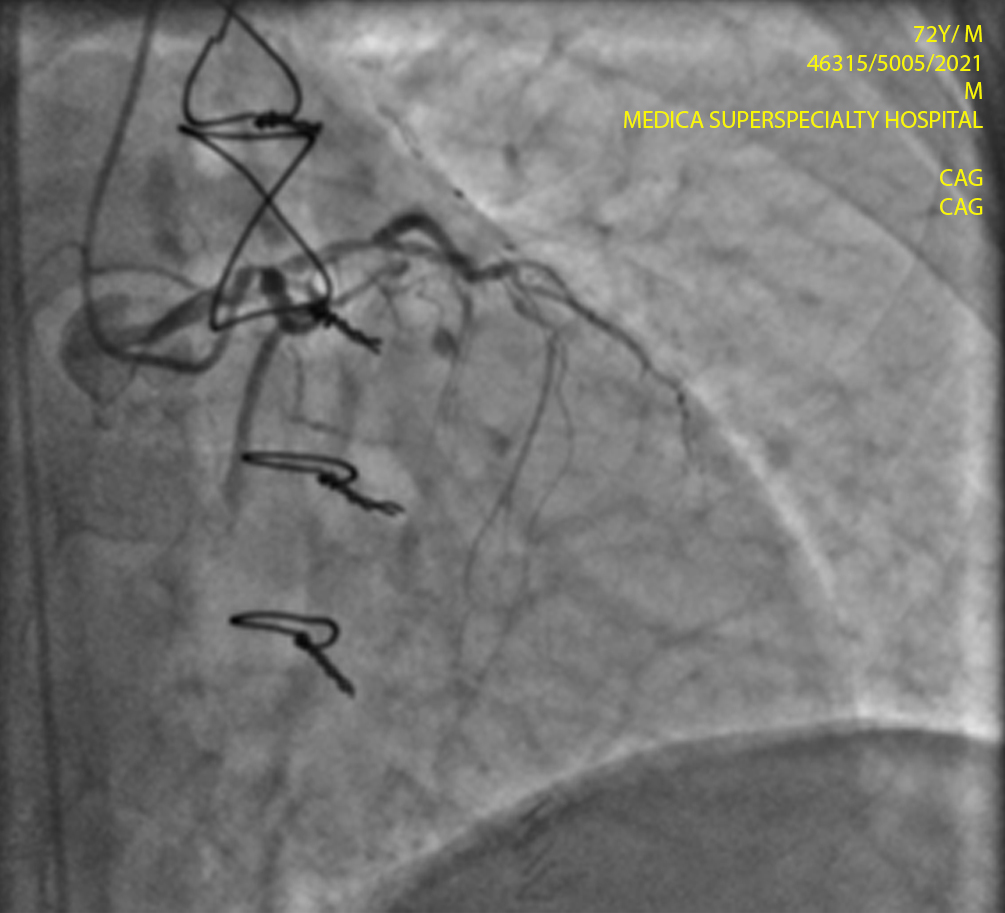
- Left Main: Distal LMCA has 80 % stenosis
- Ostial LAD has 90% stenosis. Mid LAD has total occlusion
Ramus Intermedius: NA
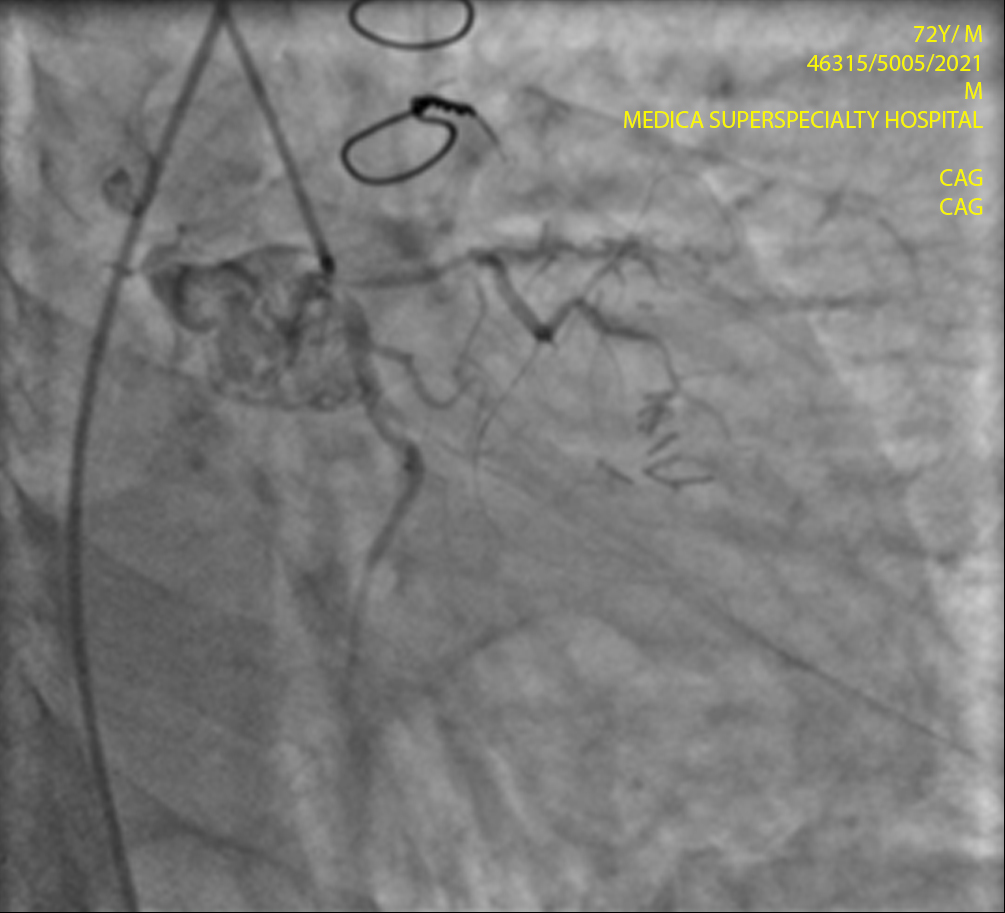
- LCX/ OM: Dominant Ostial LCX has 90% stenosis
- Non dominant. Diffusely diseased
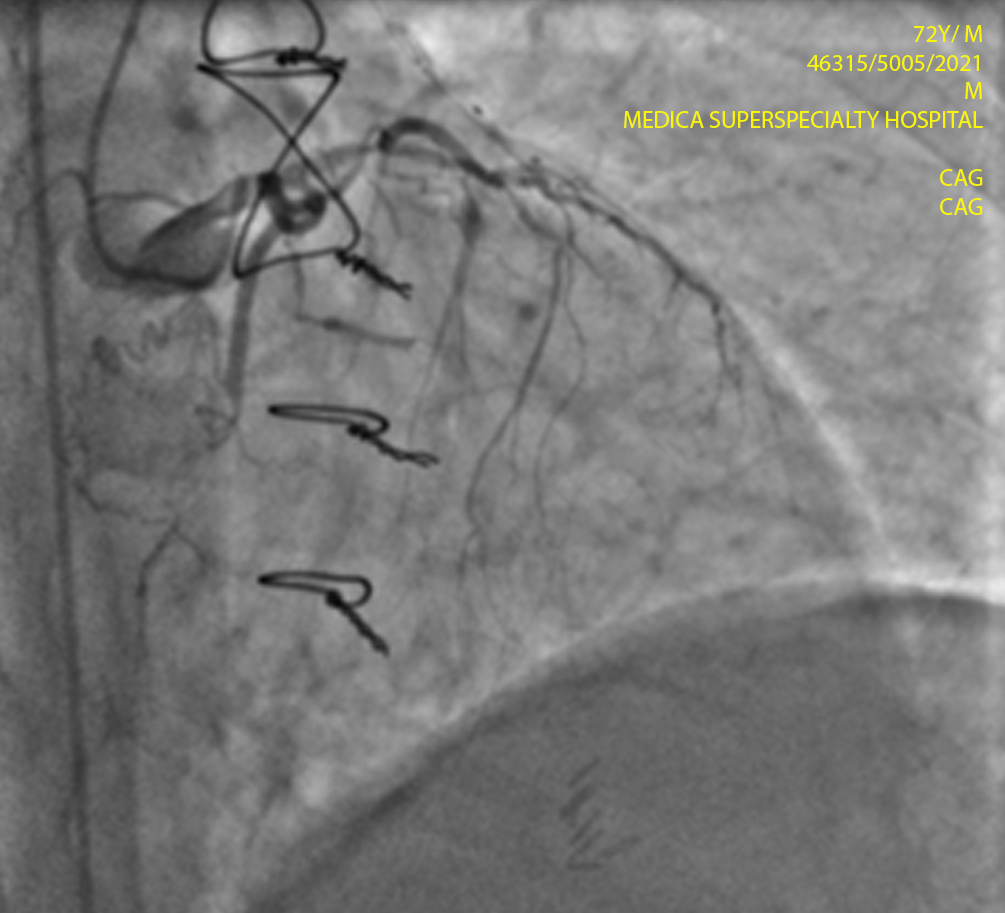
LIMA/RIMA
- LIMA-LAD-> Absent
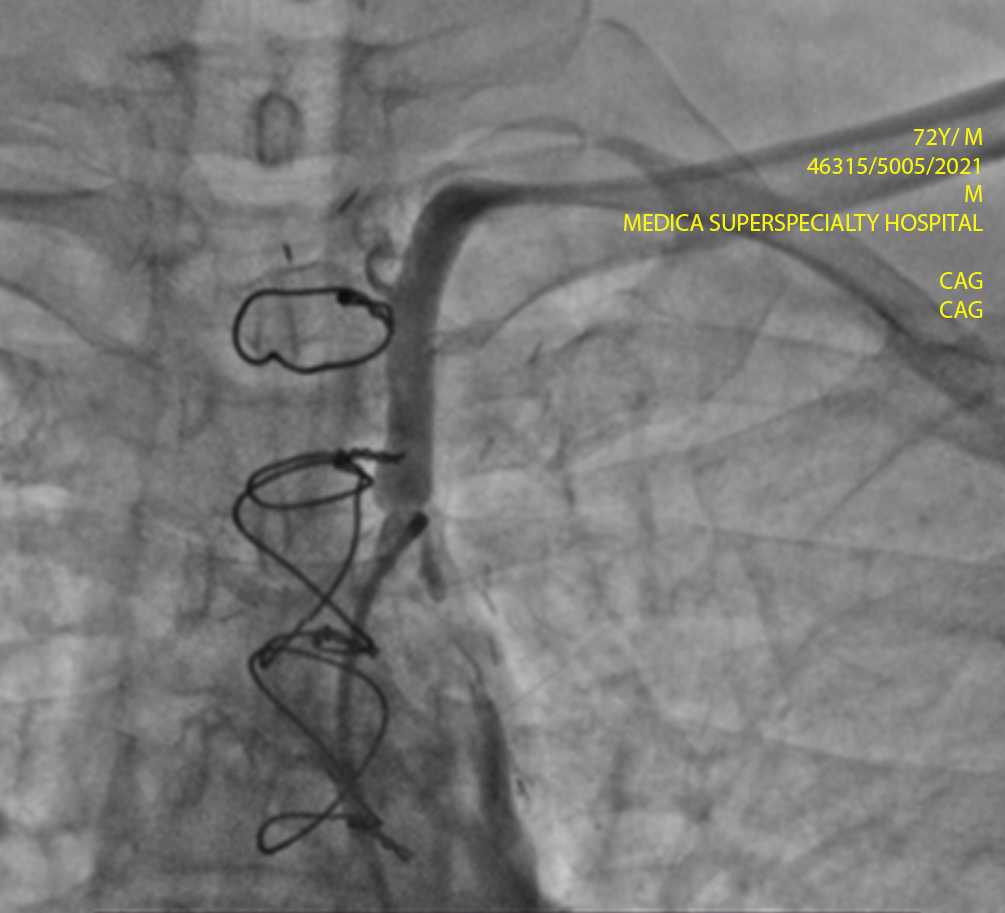
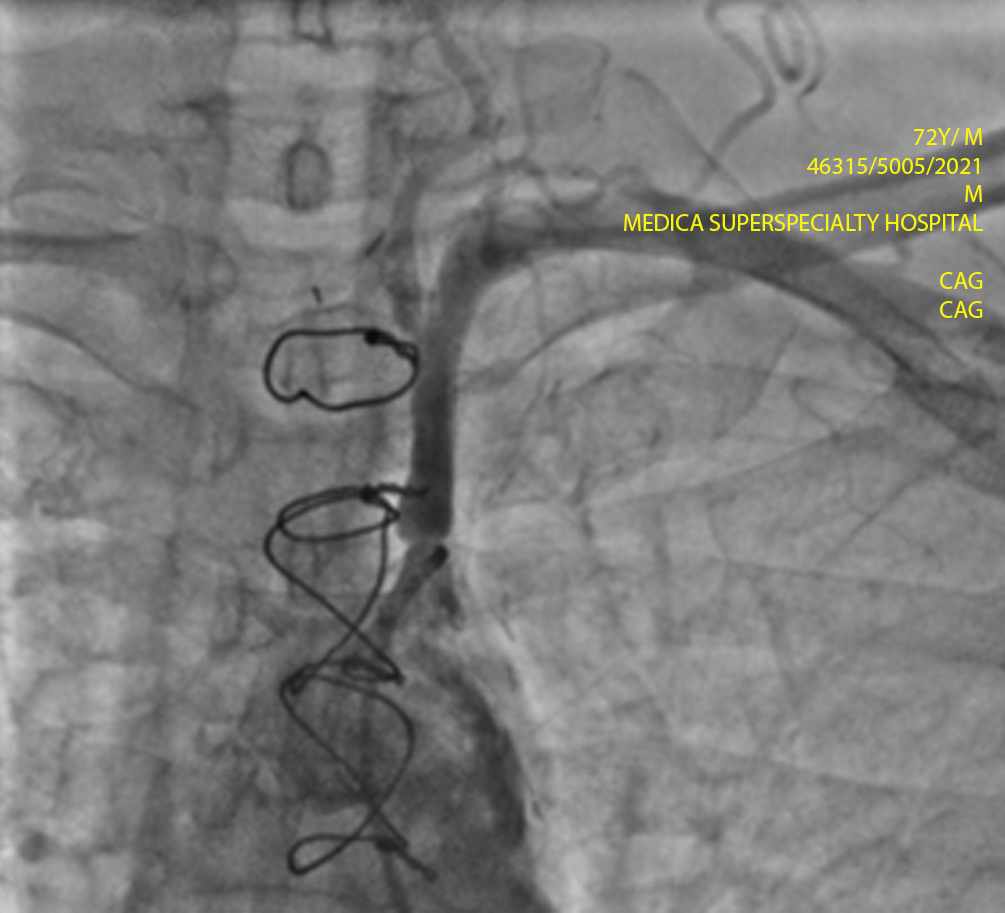
- SVG-LCX-> Patent
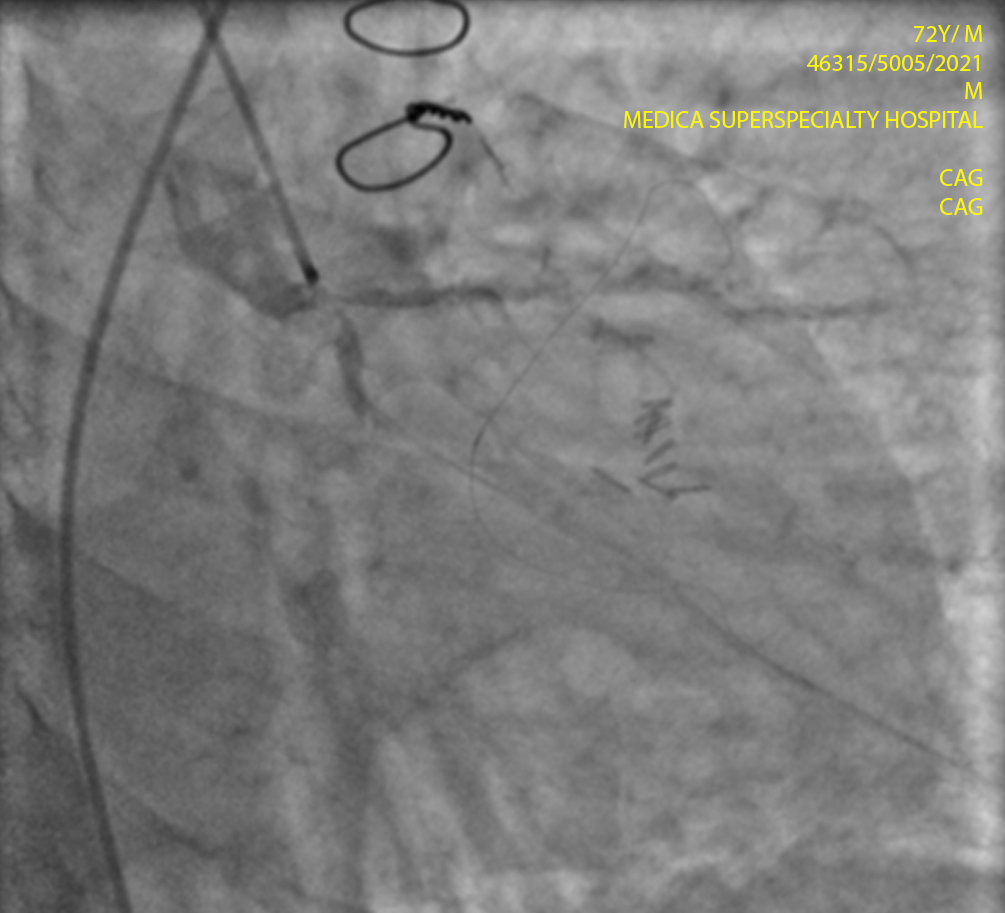
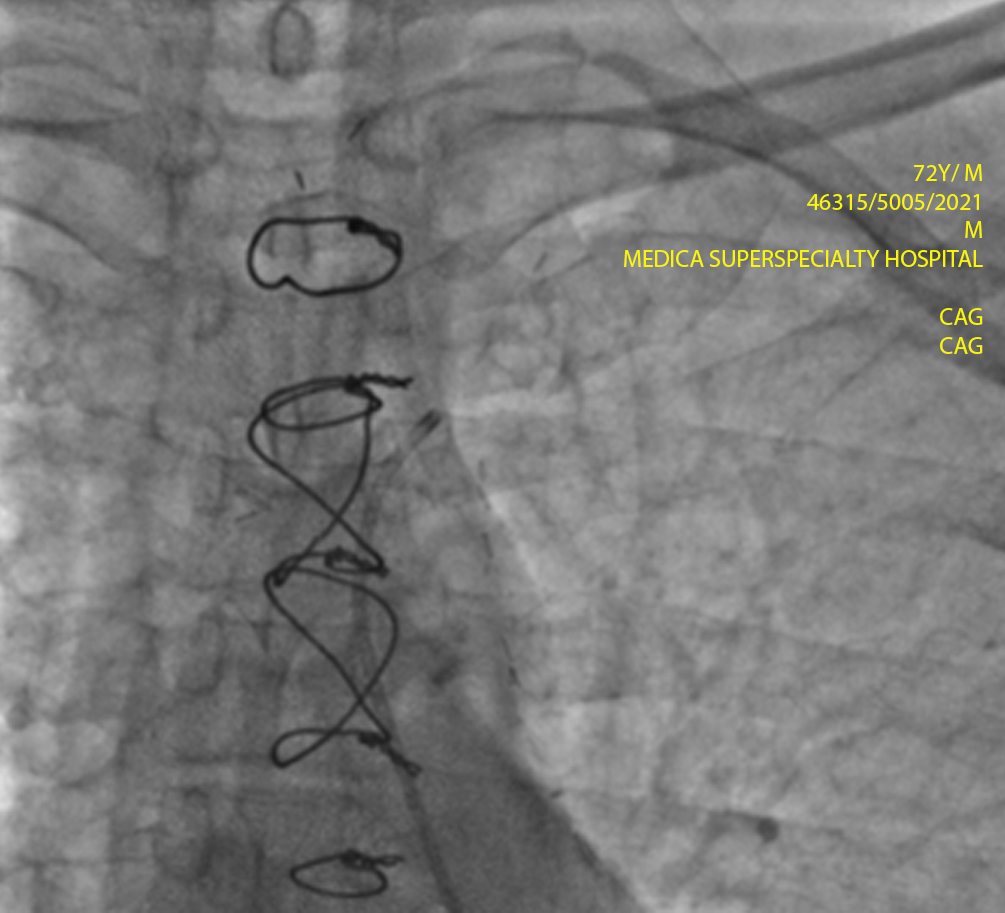
- SVG-LAD-> Discrete 90% stenosis in proximal half. Distally slow flow noted.
LV Angiogram
– NA
Renal/Angio/Carotid-Angio
– NA
Any other
– NA
Final Diagnosis
– Native triple vessel coronary artery disease. LIMA-LAD graft absent, SVG-LCX patent graft and significant disease in
SVG-LAD graft.
Recommendation
– PTCA with stenting to SVG-LAD graft
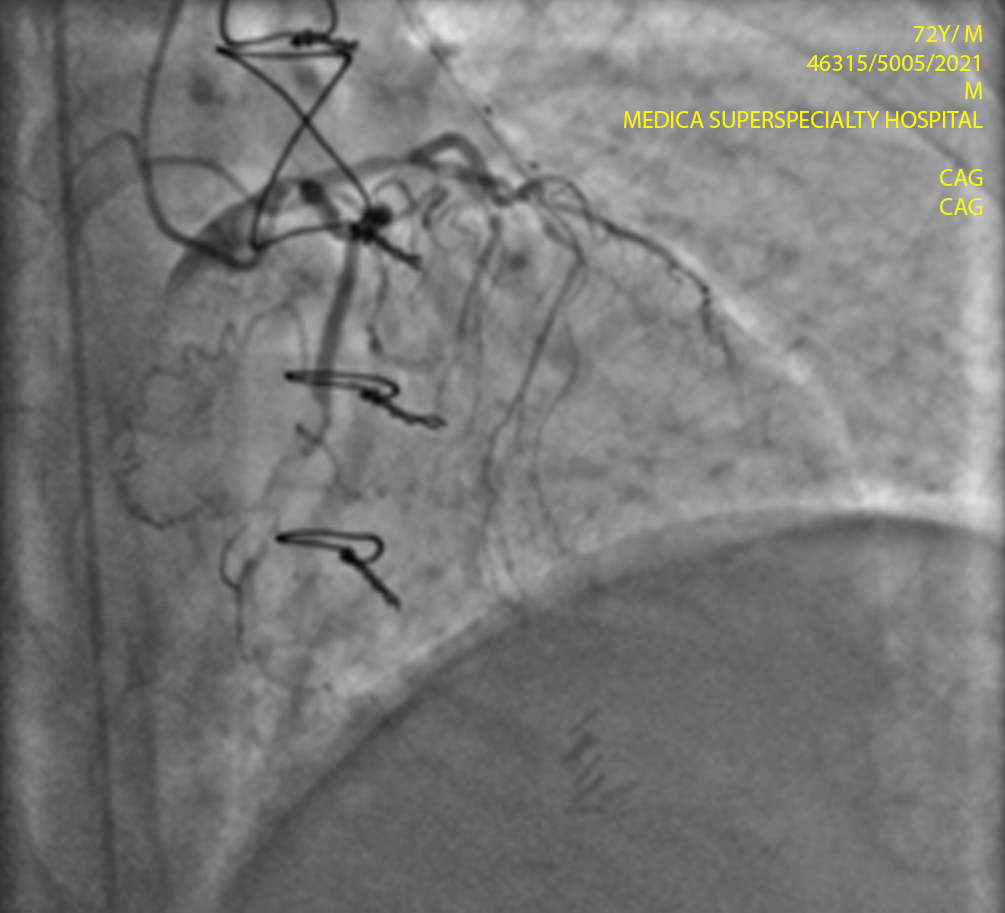
Procedure done
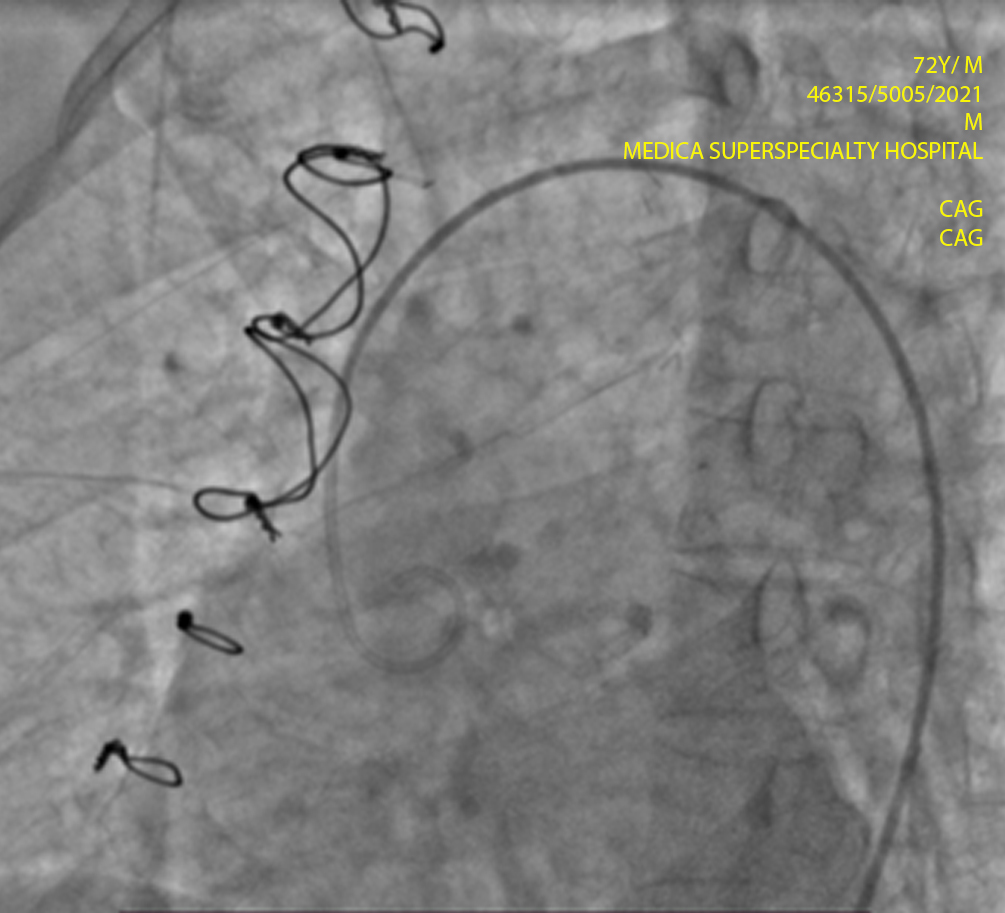
– PTCA was done through right femoral approach and good flow was achieved in SVG-LAD graft.
Procedural Details :
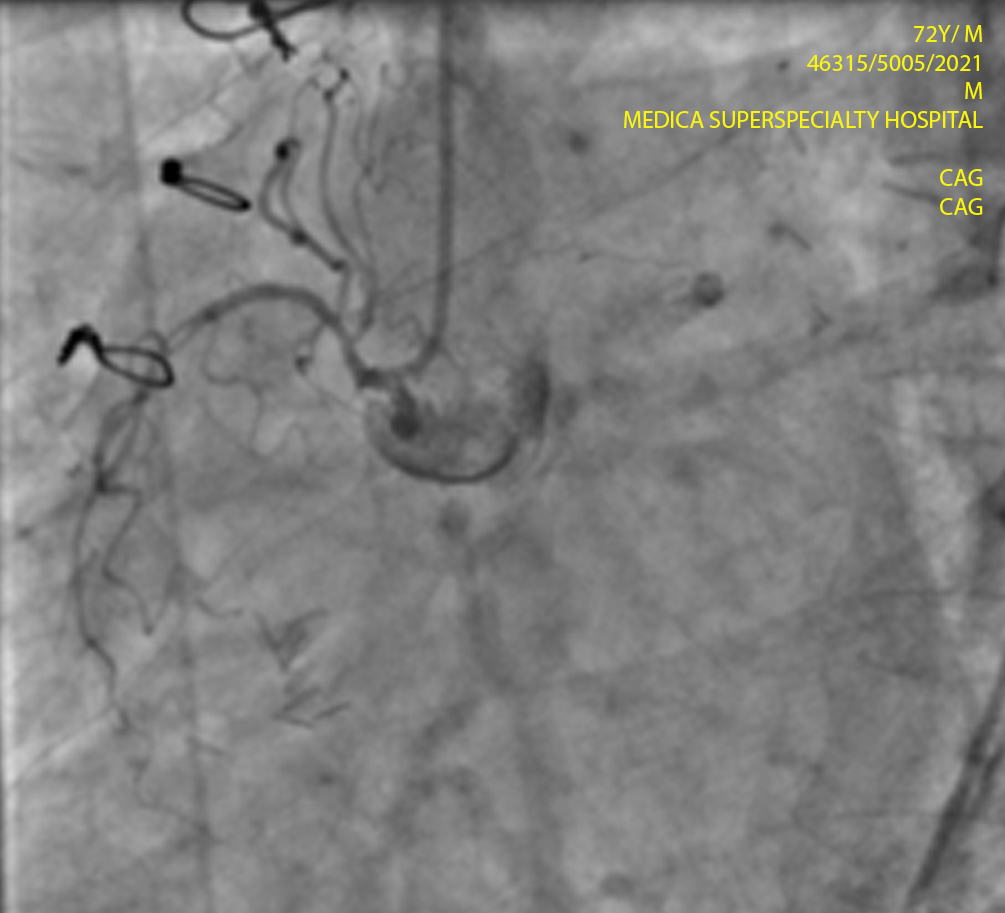
- PTCA was done through right femoral approach.
- 6F AR 1.0 guide catheter was used to engage the SVG to LAD graft.
- Asahi Sion Blue guide wire was taken to cross the lesion.
- Sequential pre dilatation was done with Ryurei 1.5 x 10 balloon at 12 atm and Ryurei 2.5 x 10 balloon at 14 atm,
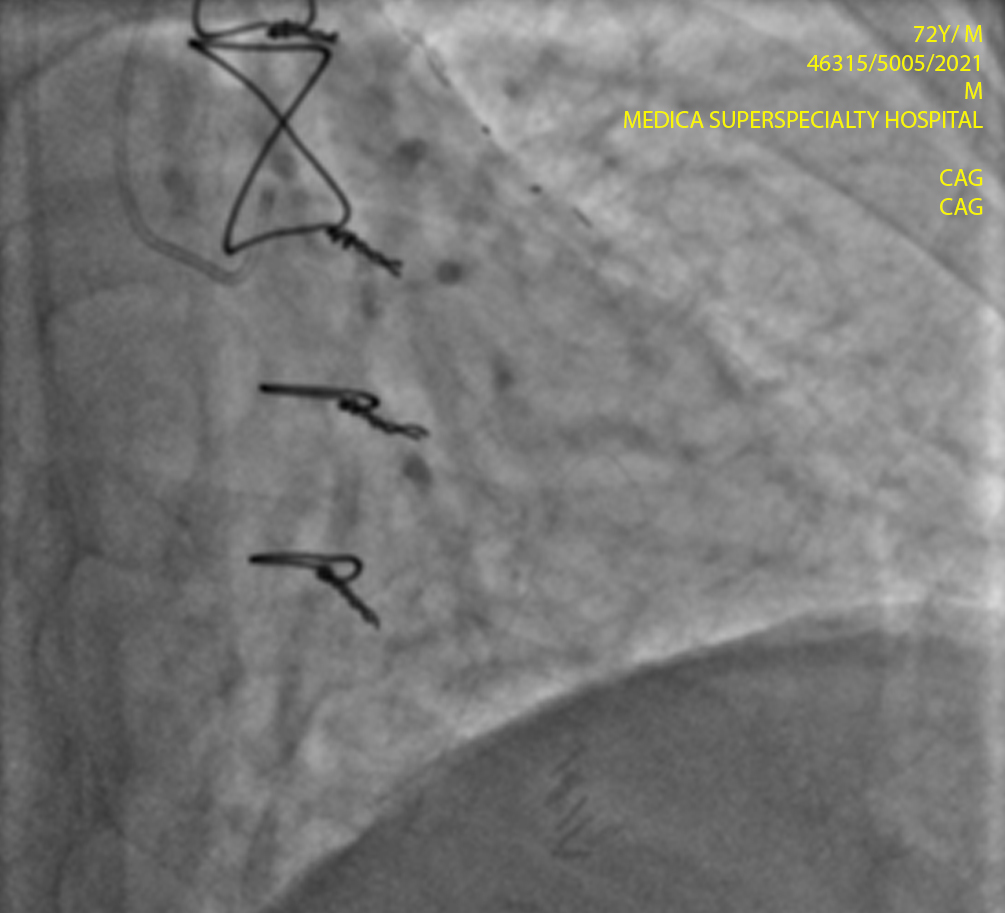
Yukon Choice PC 3.0 x 24 mm stent was deployed with the support of 6F Guidezilla supportive catheter at 12 atm. - Stent boost guided sequential post dilatation was done with balloon Apollo 3.5 x 10 at 20 atm and Apollo 4.0 x 8
balloon at 22 atm. - Post dilatation was done with high pressure balloon OPN NC 2.5 x 10 at 36 atm.
- Post stenting IVUS was done for confirming the stent apposition with 3.0F Opticross HD IVUS catheter and the
measured MSA was 5.30 mm2.
Pre-procedural findings
Details of Investigation (Findings) Post
Procedure:
ECG
- Sinus Rhythm.
- T wave inversion V1 – V4
ECHO
– Good LV systolic function
Condition at the time of discharge:
Stable
Discharge Advice:
- Tab ECOSPRIN 75 mg 1 tab once daily at 10 pm (Do not stop without doctor’s consultation).
- Tab CLOPITAB 75 mg tab twice daily at 10 am & 10 pm (Do not stop without doctor’s consultation).
- Tab ROZAVEL 40 mg 1 tab once daily at 10 pm.
- Tab FLAVEDON MR 35 mg 1 tab twice daily at 10 am and 10 pm.
- Tab KORANDIL 5 mg 1 tab twice daily at 10 am and 10 pm.
- Tab GALVUS MET (50/1000) 1 tab once daily at 10 am.
- Tab ZORYL M (1) 1 tab once daily before breakfast to continue.
- Tab CONCOR 2.5 mg 1 tab once daily at 10 am.
- Tab ESLO 2.5 mg 1 tab once daily at 10 pm.
- Tab DYTOR 10 mg 1 tab once daily at 8 am.
- Tab MUCINAC 600 mg 1 tab twice daily at 10 am and 10 pm for 5 days.
- Cap PAN-D 1 cap once daily before breakfast.
Instructions to watch for emergency:
Chest pain/discomfort, shortness of breath, syncope,
palpitation
General Advice:
- Proper medical management
- Oil, fat, salt restricted and diabetic diet
Follow-up
- Follow up after 30 days in Cardiology OPD with of CBC, FBS, PPBS, Na+, K+, Urea, Creatinine, ECG – 12 leads
reports with prior appointment. - In case of unwanted symptoms, visit Emergency department.
Discussion
Calcified non-dilatable lesions is a challenge for the interventional cardiologist. These lesions are developing
more often in the catheterization laboratory as the total complexity of interventions are increasing. Stent
under-expansion is the main risk factor for restenosis and thrombosis.1
The OPN NC balloon offers a new method of dilating lesions or under-expanded stents when other noncompliant
balloons have failed in the catheterization process. The safety of the OPN NC balloon is reasonable, even at pressures
as high as 40 atm.1
Ref: Díaz JF, Gómez-Menchero A, Cardenal R, Sánchez-González C, Sanghvi A. Extremely high-pressure dilation with a new
noncompliant balloon. Tex Heart Inst J. 2012;39(5):635-638.
Recent Comments
Ravi m
April 25, 2022 at 9:22 amNyc case & presentation
Shreya Devalkar
April 28, 2022 at 2:56 pmVery-well presented case